Talking About Symptoms
Talking About Symptoms
When you talk with your patients about their menopausal symptoms, what’s going unsaid?
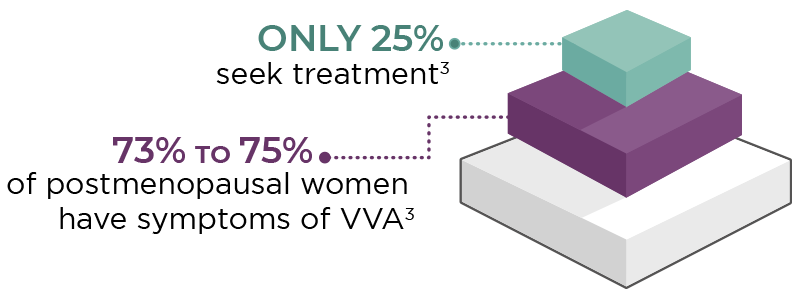
In the US, vasomotor symptoms (VMS) are among the main menopausal symptoms for which women seek treatment.1,2 In contrast, although nearly 75% of postmenopausal women experience symptoms of vulvar and vaginal atrophy (VVA), only 25% of those women seek treatment.3
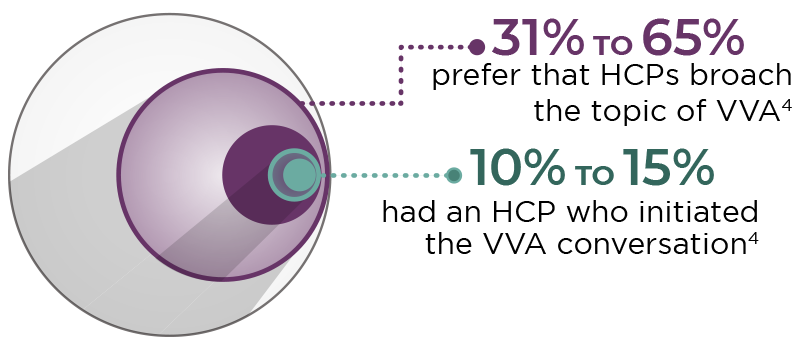
Only about half of all postmenopausal women speak at all about their vaginal symptoms with their healthcare provider (HCP). In 5 surveys (4 in the US, 1 in Europe), few participants (10%-15%) indicated that their HCP broached the topic of VVA, but many (31%-65%) would prefer that their HCP be the one to start the conversation.4

Why aren’t women talking about VVA?4
- Reluctant to talk about vaginal problems with their HCP
- Concerned about safety of hormonal treatments
- Unaware that VVA is related to menopause
- Believe they must live with VVA as part of aging
- Unaware that treatments are available
Start the conversation to help your patients become aware of and informed about their options. This technique may help patients to feel more comfortable talking about their symptoms5,6:
-
To inform and provide context, lead with a general statement.
“After menopause, many women experience vaginal dryness, itching, or pain during sex.”
-
Then offer a simple yes/no question.
"Have you had any symptoms like those?"
-
If the patient answers in the affirmative, move on to open-ended questions.
“Tell me more about your experience with these symptoms.”
VVA Symptoms
Moderate to severe symptoms of VVA due to menopause may include7
- Vaginal dryness
- Vaginal and/or vulvar irritation/itching
- Dyspareunia (vaginal pain associated with sexual activity)
Vasomotor Symptoms
VMS, including hot flashes and night sweats, are the menopausal symptoms most commonly reported to healthcare providers.1,2 During and after the transition to menopause, up to 80% of women experience moderate to severe VMS.8

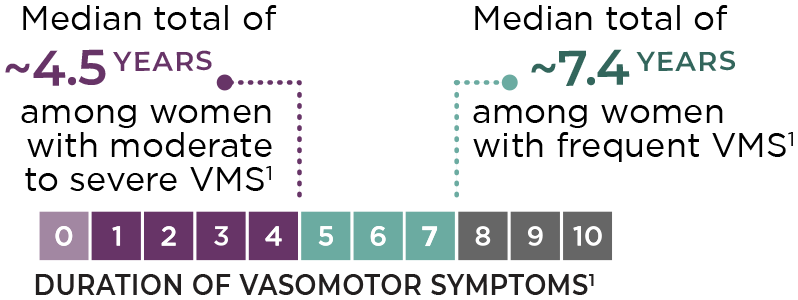
VMS may last for years. Among all women with frequent VMS, the median total duration of VMS is approximately 7.4 years, with moderate to severe hot flashes persisting a median of about 4.5 years after the last menstrual period.1,8
Duration of menopausal VMS varies greatly by race/ethnicity, with African American women experiencing VMS for the longest (a median total duration of 10.1 years).1
References: 1. Avis NE, Crawford SL, Greendale G, et al. Duration of menopausal vasomotor symptoms over the menopause transition. JAMA Intern Med. 2015;175(4):531-539. 2. Williams RE, Kalilani L, DiBenedetti DB, Zhou X, Fehnel SE, Clark RV. Healthcare seeking and treatment for menopausal symptoms in the United States. Maturitas. 2007;58(4):348-358. 3. Naumova I, Castelo-Branco C. Current treatment options for postmenopausal vaginal atrophy. Int J Womens Health. 2018;10:387-395. 4. Krychman M, Graham S, Bernick B, Mirkin S, Kingsberg SA. The women's EMPOWER survey: women's knowledge and awareness of treatment options for vulvar and vaginal atrophy remains inadequate. J Sex Med. 2017;14(3):425-433. 5. Parish SJ, Nappi RE, Krychman ML, et al. Impact of vulvovaginal health on postmenopausal women: a review of surveys on symptoms of vulvovaginal atrophy. Int J Womens Health. 2013;5:437-447. 6. Freedman MA. Perceptions of dyspareunia in postmenopausal women with vulvar and vaginal atrophy: findings from the REVIVE survey. Womens Health (Lond). 2014;10(4):445-454. 7. Food and Drug Administration. Estrogen and estrogen/progestin drug products to treat vasomotor symptoms and vulvar and vaginal atrophy symptoms—recommendations for clinical evaluation. Draft guidance. Washington, DC; US Department of Health and Human Services; January 2003. 8. Freeman EW, Sammel MD, Sanders RJ. Risk of long-term hot flashes after natural menopause: evidence from the Penn Ovarian Aging Study cohort. Menopause. 2014;21(9):924-932.